
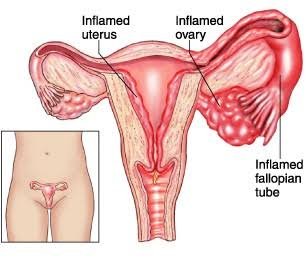
Everything you need to know about Pelvic Inflammatory Disease
PID is a clinical syndrome that results from the ascension of microorganisms from the cervix and vagina to the upper genital
Definition
Pelvic inflammatory disease (PID) is a clinical syndrome that results from the ascension of microorganisms from the cervix and vagina to the upper genital tract. PID is a serious complication of chlamydia and gonorrhea, two of the most common reportable infectious diseases and sexually transmitted diseases (STDs) in the US and around the world.
Women with PID may present with a variety of clinical signs and symptoms that range from unnoticeable or subtle and mild to severe. PID can go unrecognized by women and their health care providers when the symptoms are mild. Despite lack of symptoms, histologic evidence of endometritis has been demonstrated in women with subclinical PID.1 When present, signs and symptoms of PID are nonspecific, so other reproductive tract illnesses and diseases of both the urinary and the gastrointestinal tracts should be considered when evaluating a sexually active woman with lower abdominal pain. Pregnancy (including ectopic pregnancy) must also be excluded, as PID can occur concurrently with pregnancy.
When symptoms are present, the most common symptoms of PID are
- Lower abdominal pain
- Mild pelvic pain
- Increased vaginal discharge
- Irregular menstrual bleeding
- Fever (>38° C)
- Pain with intercourse
- Painful and frequent urination
- Abdominal tenderness
- Pelvic organ tenderness
- Uterine tenderness
- Adnexal tenderness
- Cervical motion tenderness
- Inflammation
How do women get pelvic inflammatory disease?
Women develop PID when certain bacteria, such as Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG), move upward from a woman’s vagina or cervix into her reproductive organs. PID can lead to infertility and permanent damage of a woman’s reproductive organs.
What causes pelvic inflammatory disease?
A number of different microorganisms can cause or contribute to PID. The sexually transmitted pathogens C. trachomatis and N. gonorrhoeae have been implicated in a third to half of PID cases.2-8 However, endogenous microorganisms, including gram positive and negative anaerobic organisms and aerobic/facultative gram positive and negative rods and cocci, found at high levels in women with bacterial vaginosis, also have been implicated in the pathogenesis of PID. Newer data suggest that Mycoplasma genitalium may also play a role in PID and may be associated with milder symptoms although studies have failed to demonstrate a significant increase in PID following detection of M. genitalium in the lower genital tract. Because of the polymicrobial nature of PID, broad-spectrum regimens that provide adequate coverage of likely pathogens are recommended.
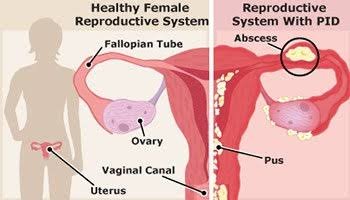
What are the complications of pelvic inflammatory disease?
Complications of PID include
- Tubo-ovarian abscess (TOA)
- Tubal factor infertility
- Ectopic pregnancy
- Chronic pelvic pain
Tubo-ovarian abscess (TOA) is a serious short-term complication of PID that is characterized by an inflammatory mass involving the fallopian tube, ovary, and, occasionally, other adjacent pelvic organs. The microbiology of TOAs is similar to PID and the diagnosis necessitates initial hospital admission. Treatment includes broad-spectrum antibiotics with or without a drainage procedure, with surgery often reserved for patients with suspected rupture or who fail to respond to antibiotics. Women infected with human immunodeficiency virus (HIV) may be at higher risk for TOA. Mortality from PID is less than 1% and is usually secondary to rupture of a TOA or to ectopic pregnancy.
Recurrent episodes of PID and increased severity of tubal inflammation detected by laparoscopy are associated with greater risk of infertility following PID. However, even subclinical PID has been associated with infertility. This emphasizes the importance of following screening and treatment recommendations for chlamydia and gonorrhea to prevent PID when possible, and promptly and appropriately treating cases of PID that do occur.
How common is pelvic inflammatory disease in the United States?
PID is a frequent and important infection that occurs among women of reproductive age. Based on data from the National Health and Nutrition Examination Survey (NHANES) 2013-2014 cycle, the estimated prevalence of self-reported lifetime PID was 4.4% in sexually experienced women of reproductive age (18–44 years). This equates to an estimated 2.5 million women in the United States with a reported lifetime history of PID diagnosis. The prevalence was highest in women at increased risk, such as those with previous sexually transmitted infections (STIs).
The significant burden of disease attributed to PID comes predominantly from the long-term reproductive sequelae of tubal infection: tubal factor infertility, ectopic pregnancy, and pelvic adhesions, which can lead to chronic pelvic pain. Our knowledge of the longitudinal outcomes for affected women who experience PID is primarily derived from data published using a Scandinavian cohort of inpatients diagnosed with PID.19 Data from this study indicated that those women with PID were more likely to have ectopic pregnancy (6 times increased rate), tubal factor infertility (ranging from 8% after the first episode to as high as 40% after three episodes) and chronic pelvic pain (18% following one episode).
How is pelvic inflammatory disease diagnosed?
The wide variation in symptoms and signs associated with PID can make diagnosis challenging. No single historical, physical, or laboratory finding is both sensitive and specific for the diagnosis of PID. Clinicians should therefore maintain a low threshold for the diagnosis of PID, particularly in young, sexually active women.
Criteria have been developed for the diagnosis of PID.
Presumptive treatment for PID should be initiated in sexually active young women and other women at risk for STDs if they are experiencing pelvic or lower abdominal pain, if no cause for the illness other than PID can be identified, and if one or more of the following minimum clinical criteria are present on pelvic examination:
- cervical motion tenderness
or - uterine tenderness
or - adnexal tenderness.
The requirement that all three minimum criteria be present before the initiation of empiric treatment could result in insufficient sensitivity for the diagnosis of PID. After deciding whether to initiate empiric treatment, clinicians should also consider the risk profile for STDs.
More elaborate diagnostic evaluation frequently is needed because incorrect diagnosis and management of PID might cause unnecessary morbidity. For example, the presence of signs of lower-genital–tract inflammation (predominance of leukocytes in vaginal secretions, cervical exudates, or cervical friability), in addition to one of the three minimum criteria, increases the specificity of the diagnosis. One or more of the following additional criteria can be used to enhance the specificity of the minimum clinical criteria and support a diagnosis of PID:
- oral temperature >101°F (>38.3°C);
- abnormal cervical mucopurulent discharge or cervical friability;
- presence of abundant numbers of WBC on saline microscopy of vaginal fluid;
- elevated erythrocyte sedimentation rate;
- elevated C-reactive protein; and
- laboratory documentation of cervical infection with N. gonorrhoeae or C. trachomatis.
Most women with PID have either mucopurulent cervical discharge or evidence of WBCs on a microscopic evaluation of a saline preparation of vaginal fluid (i.e., wet prep). If the cervical discharge appears normal and no WBCs are observed on the wet prep of vaginal fluid, the diagnosis of PID is unlikely, and alternative causes of pain should be considered. A wet prep of vaginal fluid also can detect the presence of concomitant infections (e.g., BV and trichomoniasis).
The most specific criteria for diagnosing PID include:
- endometrial biopsy with histopathologic evidence of endometritis;
- transvaginal sonography or magnetic resonance imaging techniques showing thickened, fluid-filled tubes with or without free pelvic fluid or tubo-ovarian complex, or Doppler studies suggesting pelvic infection (e.g., tubal hyperemia); or
- laparoscopic findings consistent with PID.
A diagnostic evaluation that includes some of these more extensive procedures might be warranted in some cases. Endometrial biopsy is warranted in women undergoing laparoscopy who do not have visual evidence of salpingitis, because endometritis is the only sign of PID for some women.
A test for human immunodeficiency virus (HIV) is also recommended. A pregnancy test should always be performed to exclude ectopic pregnancy and because PID can occur concurrently with pregnancy. When the diagnosis of PID is questionable, or when the illness is severe or not responding to therapy, further investigation may be warranted using other invasive procedures (endometrial biopsy, transvaginal ultrasonography, magnetic resonance imaging, or laparoscopy).
How is pelvic inflammatory disease treated?

PID is treated with broad spectrum antibiotics to cover likely pathogens. Several types of antibiotics can cure PID. Antibiotic treatment does not, however, reverse any scarring that has already been caused by the infection. For this reason, it is critical that a woman receive care immediately if she has pelvic pain or other symptoms of PID. Prompt antibiotic treatment could prevent severe damage to the reproductive organs.
Recommended treatment regimens can be found in the 2021 STI Treatment Guidelines. Health care providers should emphasize to their patients that although their symptoms may go away before the infection is cured, they should finish taking all of the prescribed medicine. Additionally, a woman’s sex partner(s) should be treated to decrease the risk of re-infection, even if the partner(s) has no symptoms. Although sex partners may have no symptoms, they may still be infected with the organisms that can cause PID.
In certain cases, clinicians may recommend hospitalization to treat PID. This decision should be based on the judgment of the health care provider and the use of suggested criteria found in the 2021 STI Treatment Guidelines. If a woman’s symptoms continue, or if an abscess does not resolve, surgery may be needed.
How can clinicians manage PID?
A critical component to management is short-term follow-up, especially in the adolescent population. Since many adolescent women rely on outpatient services for the evaluation and treatment of STD symptoms, the need for a low diagnostic and management threshold for PID is even more critical, as the likelihood for additional follow-up care is low.
What should a patient do after being diagnosed with pelvic inflammatory disease?
A patient should abstain from sexual intercourse until she and her partner(s) have completed treatment. Female latex condoms are also an option if a woman prefers them or if her male partner chooses not to use male condoms. Women who are told they have an STD and are treated for it should notify all of their recent sex partners so they can see a health care provider and be evaluated for STDs.
The diagnosis of PID provides an opportunity to educate adolescent and young women about prevention of STDs, including abstinence, consistent use of barrier methods of protection, immunization, partner evaluation and treatment, and the importance of receiving periodic screening for STDs and HIV.
How can pelvic inflammatory disease be prevented?
Latex condoms may reduce the risk of PID by preventing STDs. Since STDs play a major role in PID, screening of women at risk for infection and treatment of infected women and their sex partners can help to minimize the risk of PID. Screening of young sexually active women for chlamydia has been shown to decrease the incidence of PID.
The United States Preventive Services Task Force recommends annual chlamydia and gonorrhea screening in women younger than 25 years25 and CDC recommends that providers screen the following populations for chlamydia and gonorrhea: all sexually active women younger than 25 years, as well as older women with risk factors such as new or multiple sex partners, or a sex partner who has a sexually transmitted infection.
Credit: Detailed Fact Sheet, Center for Disease Control & Prevention, US